More than 400 years after the first enslaved people were brought to our country, racism continues to batter the health of Black Americans. Consider these U.S. statistics that reveal profound health inequities between Black and white Americans:
- Black mothers die at four times the rate of white mothers around the time of childbirth; Black newborns die at three times the rate of white newborns.
- In Minnesota, 33% of Black children grow up in poverty compared to 6% of white children.
- Black women are 40% more likely to die of breast cancer than white women.
- Black Americans are 80% more likely to be diagnosed with diabetes than white Americans.
Open and obvious signs of racism, along with more subtle microaggressions — such as glances and whispered words — can stress the physical and psychological health of Black people to a life-threatening degree. University of Michigan’s Arline Geronimus labeled this cumulative stress process “weathering” and feels it may explain, for example, why Black teenage mothers have better birth outcomes than Black women in their 20s-30s who have lived longer in a racist society.
Recent research also points to the chronic stress of racial discrimination as a possible factor in why Black Americans suffer diminishing cognition and Alzheimer’s disease at a rate two to three times higher than white Americans.
The types of racism that are often unseen and unheard — structural, systemic, and institutionalized racism — are equally vicious and quietly erode chances for Black people to get ahead and to be healthy.
Recent research also points to the chronic stress of racial discrimination as a possible factor in why Black Americans suffer diminishing cognition and Alzheimer’s disease at a rate two to three times higher than white Americans.
The system isn’t broken — it was built this way.
Structural racism was built into the systems that organize our society, such as law enforcement, banking, education, city planning, medicine, and housing, as well as organizations that give power and provide a sense of belonging.
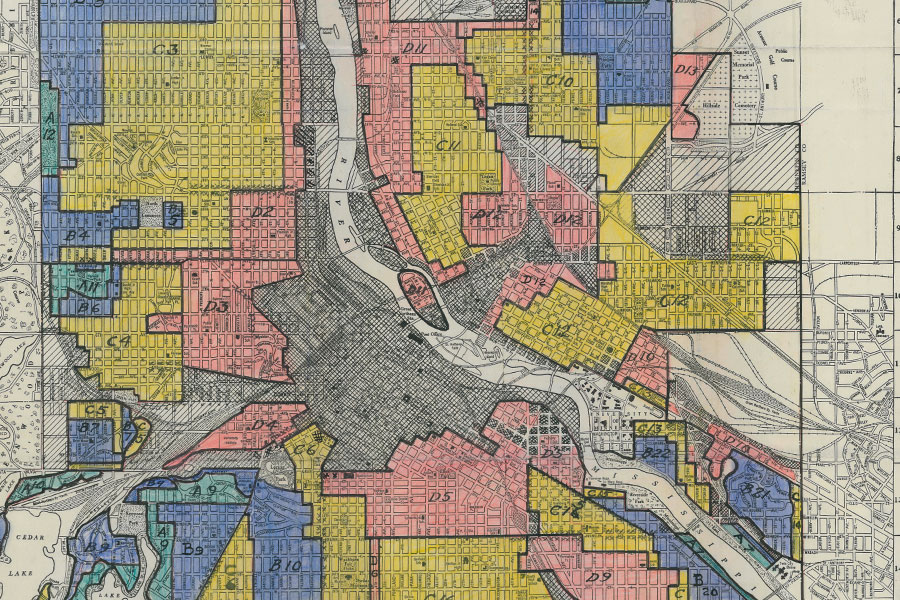
One example of structural racism is redlining, so named for the process of shading in red parts of a city that were deemed undesirable for investment by banks and other businesses because of what a 1934 Home Owners’ Loan Corporation document calls a “gradual infiltration of negroes and Asiatics.”
Today’s city neighborhoods still reflect the practice that has kept Black home ownership stifled, hobbling intergenerational wealth. According to a study from Redfin, just 25 percent of Black families own a home in Minneapolis compared with 76 percent of whites — the widest gap in U.S. cities with more than 1 million people.
And redlining continues to have an impact on health. For example, a recent study shows that the heat index in redlined areas far exceeds that in other parts of a city, because of fewer trees and more concrete. It found that Minneapolis, Portland, and Denver had temperature differentials over 10 degrees Fahrenheit between historical redlined areas and other parts of the cities. High heat exacerbates medical conditions and affects air quality, causing health impacts that can span generations. Redlining’s legacy is also evident in fewer grocery stores, safe places to walk or bike, and other health-promoting resources in certain neighborhoods.
Racism as a public health crisis
The killing of George Floyd on May 25 and its aftermath brought the many health impacts of racism erupting to the surface of an America ignorant or in denial. Media coverage of the disproportionate number of Black people who die of COVID-19 is drawing attention to racial disparities in health. (In Minnesota, Black Americans account for 6% of the population, but 14% of COVID-19 cases and 33% of deaths.)
Many cities, counties, and states across the U.S. have declared racism a public health emergency or crisis. Joining them are the American Academy of Pediatrics, American College of Emergency Physicians, and American Medical Association, which called “racism in its systemic, structural, institutional, and interpersonal forms…an urgent threat to public health.”
Googling “racism as a public health crisis” brings up pages upon pages of results, most all dating from March 2020. Public health has always known that there were differences in the health of Black and white Americans, but tended until recently to attribute those differences to personal behavior, culture, and genetics, just as medicine did (and still often does). And although public health looks extremely closely at the “social determinants of health” — food, health care, housing, education, etc. — it has not closely examined the impact of structural racism.
“When it came to the effects of structural racism [on health], we knew a lot from lived experiences, but we weren’t naming it and we certainly weren’t measuring it in public health research,” says Rachel Hardeman, School of Public Health Associate Professor and Blue Cross Endowed Professor of Health and Racial Equity.
Through a review of public health literature from 2002 to 2015, Hardeman found only 25 articles out of thousands that mentioned institutionalized racism and only 16 of those 25 identified it as a core contributor to health inequities.
What’s the role of public health?
Hardeman’s review shows that public health has not traditionally named structural racism as the extra layer of harm contributing to already poor social determinants of health in the Black community, and as causing many of those poor social determinants in the first place.
Public health’s history when it comes to Black Americans is deeply tied to the “Tuskegee Study of Untreated Syphilis in the Negro Male,” which the Public Health Service conducted with the Tuskegee Institute from 1932 through 1972. For 40 years, researchers examined the progress of syphilis in poor Black men without ever treating them for the disease even after penicillin was found to be a cure. By the time the study ended, 28 men had died from syphilis, 100 more had died from related complications, at least 40 spouses had been diagnosed with syphilis, and 19 of the men’s children had been born with the disease.

Hardemen found in a recent study that the harm generated by the Tuskegee study continues in “peripheral trauma” that affects a community’s mental and physical health even though its members may not have been directly involved. Black Americans, in general, distrust the medical system and that leads, in part, to entrenched health disparities. Black Americans are highly reluctant to enroll in clinical trials, and polls on who might or might not get a COVID-19 vaccine show Black Americans to be more hesitant than whites or Hispanics.
“…we have to name racism. We have to stop being afraid of the R-word. We have to call it when we see it. We have to say this is what racism is. This is what it looks like.”
Georges Benjamin
Given public health’s role in contributing to health inequities in Black Americans via the Tuskegee study and the field’s lag in examining the effects of structural racism, how can it meet this crisis and give following generations of Black Americans a chance for healthier lives?
“One of the things I’ve learned in practicing medicine is the first thing you have to do is identify the problem,” says Georges Benjamin, physician and head of the American Public Health Association, in the SPH podcast Health in All Matters. “And so we have to name racism. We have to stop being afraid of the R-word. We have to call it when we see it. We have to say this is what racism is. This is what it looks like. We have to understand what it is. Then we have to ask ourselves how does it operate here? … [T]hen we can decide on crafting meaningful solutions. But you cannot solve a problem until you know you have a problem, and everyone accepts that the problem is real.”
Nathan Chomilo, a pediatrician and Minnesota’s Medical Director for Medicaid, thinks public health researchers and practitioners should look at overall health through a wider lens and from the viewpoint of its community partners.
“Health is affected by access to education, nutrition, childcare, paid leave, fair wage and economic inequality,” Chomilo says. “Let’s face disparities to co-create health solutions, sharing power and stewardship of the resources so that communities can enact solutions themselves. We can’t simply go back to normal [pre-George Floyd days] because normal wasn’t working for so many of our communities and our neighborhoods.”
Hardeman and other SPH faculty are raising research questions about structural racism and population health and designing studies to yield empirical data. Some are tackling such issues as race and quality of life in nursing homes; how to improve relationships between young Black men and police; and if prenatal care use varies across Black women with light brown, medium brown, or dark brown complexions.
As schools of public health across the country are examining their own histories and need for action around race and racism, the entire field of public health is digging deep to examine the role it must play. If public health is built on the foundation that health is a human right, it is now the time, like no other, to make sure that foundation is strong.

If not now, when?
In the first series of the SPH podcast Health in All Matters, we tackled the evolving pandemic and the many issues it brings into question. Series 2 focuses on racism and public health — their complex history, pivotal present, and awakened future. Through personal stories and expert commentary, we highlight the people and organizations who fight for racial justice, and explore how public health can support their work and do its part to drive structural change.


